A PPC Seminar Built for Sports Chiropractors
by Dr. Chad Peters
This is not a traditional PPC article.
This writeup was built specifically for sports-minded chiropractic students, athletic trainers, and sports med. doctors who work with athletes and build meaningful careers in sports medicine.
It is not a technique manual. It is not a protocol.
It is a collection of ideas and systems that shape how I approach athletes, injuries, and human performance.
This seminar lives in the overlap between sports medicine and human performance, because that overlap is where the best outcomes occur.

Most practitioners eventually choose one side or the other. Some become injury doctors. Others become performance coaches.
I never separated the two.
For most of my career, I have lived in the middle ground between them.
Where This System Came From


My wife and I built our practice together in a sports-based but still, community setting. (basically, all clients get sports based protocols)
Over the past two decades I have worked with a little over 33,000 patient cases, and that level of exposure changes how you see patterns in the human body.
Experience matters.
Einstein once said that information is not the same thing as knowledge, and knowledge is not the same thing as understanding. True understanding comes from experience. After enough cases, the body stops looking random and begins to look systematic.
Patterns become visible.
That experience was heavily influenced by chiropractic training, but also by time spent working in the professional sports environment. Those experiences changed the way I approach injuries and treatment.
Professional athletes expect results quickly, but they also expect to return to full function. The standard is not partial recovery. The standard is near 100 percent function AND as fast as possible.
That expectation gave me what I would describe as an athletic trainer mindset. I am always thinking in terms of return to play, at a high level – not simply reduction of symptoms.
Writing “Unlocking Athletic Potential”
While writing Unlocking Athletic Potential, I spent a great deal of time studying what actually improves athletic performance.
The intent of the book is to put to rest the ideas in high school athletics that are incorrect foundations:
How much do you weigh?
How strong are you?
Those factors matter. They always will.
But they are not the most important factors.
Not even close. Closer to the ninth and tenth metrics.
Strength and bodyweight influence performance, but they do not define it. When you dig deeper into what actually separates modern elite athletes, the most consistent factor is how well the body moves and transfers force.
That realization shaped the way I see both performance and injury.
The Three Big Engines
Over time it became clear that the greatest return on investment in the human body comes from what I call the three big engines:
-
The hips
-
The ankles/feet
-
The shoulders
When those engines function well, performance improves. When those engines function poorly, compensation begins. Many injuries are simply the visible result of an engine that is not doing its job.
One of the most important observations I have made over the years is that the same changes that improve performance often reduce pain.
That is because both processes are built around optimization.
When movement improves, tissues tolerate load better. When tissues tolerate load better, injuries become less likely and recovery becomes faster.
Performance and injury treatment are not separate conversations. They are the same conversation viewed from different angles. It’s Perspective that matters most – and today I want to give you many perspectives.
Perspectives that Changed my Treatment Protocols
– The Joint-by-Joint Approach
The body does not operate as isolated joints.
Force moves through chains of motion. When one joint fails to contribute, another joint absorbs the extra demand. I often describe this as a kinetic bleed-out, where force leaks from the system and overload accumulates somewhere else.
This way of thinking leads naturally to joint-by-joint evaluation. If a knee hurts, the knee still matters, but the hip and ankle matter just as much. If the shoulder is injured, the thoracic spine and scapular control often determine the outcome.
Looking at isolated joints alone restores normal function. Looking at systems restores performance.
– “Stability Is Not Strength” and the 14+ Factors of Fitness
One of the most persistent misunderstandings in rehabilitation is the assumption that we should loosen tight muscles and strengthen injury.
Traditional models often describe rehabilitation as stretching what is tight and strengthening what is weak. While that model has value, it is vastly incomplete.
Stability improves best through stable demands placed on the nervous system. Strength training overlaps with stability training, but it is rarely the most efficient way to develop control.
In the same way, flexibility alone rarely solves mobility problems. 4 version of tight link
Mobility is a system-level characteristic involving joints, muscles, and neurological control.
Think: The Athletic Club Mindset vs. Actual Performance Factors
Matching the tool to the problem matters. Precision always outperforms volume.
– Changing the Language
Language shapes thinking, and thinking shapes practice. I want to change how coaches, and you THINK about the body.
Over time I have found that certain “word swaps” improve communication and understanding, particularly when working with athletes and coaches.
Flexibility is often a muscle-centered concept. Mobility is a more accurate description of joint system function. In our setting we often go one step further and use the word unlock, because athletes respond better to that language.
Instead of warmups, we talk about unlocking the body. (modern Warmup link)
Instead of dynamic warmups, we talk about speed preparation.
Instead of treatment, we talk about optimization.
These are not marketing terms. They are thinking tools that help align communication between practitioners and coaches.
– Return to Play Instead of Time Off
One of the most important shifts in thinking is moving from time-based rehabilitation to function-based rehabilitation. or better stated “Injured vs. 100%.“
I do not want a rest prescription.
I want a return-to-play protocol – Time alone does not restore performance. Two weeks of rest does not mean an athlete is ready to compete. Function must be restored before return to play decisions are made.
This mindset comes directly from working with athletes, where availability and readiness matter as much as diagnosis.
but…
– Injury “Threat” Phase
The earliest phase of injury is best understood as a state of threat.
The body perceives danger. Inflammation increases. Protective patterns emerge. Repeatable Predictable Patterns.
Understanding this phase changes how treatment begins. Early intervention is not always about range of motion or strengthening. The first goal is often calming the threat response and helping the system regain a sense of safety.
This perspective influences how I think about neurological input and even basic treatment decisions such as when to use ice or heat. and why I still love EMS. The goal is not simply to reduce symptoms but to guide the nervous system a better direction.
More detailed discussions of these ideas are available in the PPC articles on ice and electrical stimulation.
– Decompression and Compression
Treatment trends often move faster than understanding.
There was a period when “stretch” dominated rehabilitation thinking. Creating space and unloading tissue can reduce symptoms and improve comfort. Great idea.
And then in 2010 an amazing confluence of systems emerged. almost a 180 to conventional treatments and with it came dozens of new tools: Crossfit, IASTM tools, Arrosti, Positional Release, Active Release, Deep SLOW hard tissue work.
Again in 2016 and amazing boost for our professions, but an atomic bomb for recovery, reasoning, and decision making.

Modern practioners have so many options for treatment. We all have our favorites but often incorrectly defer to “I am going to throw everything I have at this athlete.”
Athletes land, cut, accelerate, and decelerate under load. Successful rehabilitation must prepare athletes to tolerate compression as well as benefit from decompression.
The real question is not which method is better. The real question is which input the athlete needs at that moment.
– Kinesthetic Dyslexia
One risk of modern treatment environments is overwhelming the nervous system with too many inputs.
Scraping, cupping, taping, stretching, activation work, decompression, adjustment, and stimulation can all be useful tools. When applied without clear purpose, however, they create conflicting signals.

I describe this state as kinesthetic dyslexia, where the nervous system receives so many messages that integration becomes difficult. At best it is slow. At worst it increases THREAT and you are in essence , starting over each visit.
Athletes feel worked on and we feel like we’re doing work but the client is not becoming more functional.
Precision almost always produces better results than volume.
The Skin is the Map for the Brain
One of the ideas that most changed the way I treat athletes is understanding that the skin and superficial fascia form a major communication network between the body and the brain. Improving the quality of sensory input often improves movement faster than stretching or strengthening alone.
Key ideas to explore:
-
Kinesiology Tape as a Sensory Signal Booster
Tape improves the clarity of sensory information being sent to the brain rather than mechanically forcing change. -
Improving Proprioception
Better sensory feedback improves awareness of movement and position, which often improves coordination and control. -
Pain Modulation and Threat Reduction
Sensory input from the skin can reduce perceived threat and allow movement to return more naturally. -
Fluid Movement and Surface Decompression
The lifting effect of tape can improve superficial circulation and help restore normal fluid movement. -
Decompression and the Rebound Effect
Stretch and recoil at the skin surface can reduce pressure on superficial nerves and irritated tissues. -
Neurological Reset
Consistent sensory input can help the brain reorganize movement patterns after injury. -
The Google Maps Analogy
Clearer sensory input sharpens the brain’s picture of the body and improves movement decisions.
The Scientific Method
At its core, good clinical work follows a simple pattern:
Observe. – Form a hypothesis – Test the hypothesis – Measure the response.
Adjust and retest. – (we forgot about this!)
This process happens continuously in a thoughtful practice. The scientific method is not an academic exercise. It is the daily workflow of a clinician who is paying attention.
for us – “Are you better, worse or the same?”
Be a Detective
The most important idea of this entire seminar is simple.
Be a detective.
Do not settle for naming the injury. Solve the mechanism. Follow the clues. Think in systems. Choose tools intentionally.
The best practitioners are not the ones with the largest toolboxes.
They are the ones who understand how and when to use what they have.
That mindset is what connects sports medicine with human performance, and it is what ultimately produces the best outcomes for athletes.
Hour 2 –
Detective Work and Case Thinking
The second half of this seminar is built around case thinking.
I have always believed that clinicians learn best through real scenarios rather than abstract protocols. Protocols produce technicians. Case thinking produces decision makers.
Every athlete is a case to be solved.
Each case involves mechanisms, tolerance levels, sequencing patterns, and environmental demands. The practitioner’s role is to gather clues and build a working hypothesis.
That process looks very similar to detective work.
Observation comes first. Tools come later.
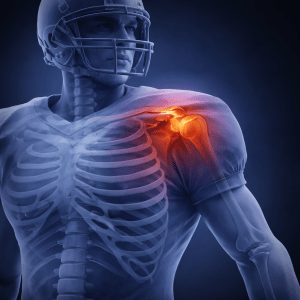
The Shoulder Case

Overhead athletes provide a clear example of system-based thinking. Shoulder pain is rarely limited to the rotator cuff. Scapular control, thoracic mobility, and force sequencing often determine the outcome.
When the surrounding system improves, shoulder symptoms often improve alongside performance.
Bicep Tendon Complex (often with a rib component)
The Low Back and Hip Case

Low back pain in athletes frequently reflects a problem in the hip. Loss of rotation, poor glute activation, and reduced stability create overload patterns that eventually appear in the lumbar spine.
Restoring hip function often reduces back symptoms while improving performance capacity.
2 cases – disc strain – hip and low back combo
The Syndesmosis Ankle Case

Syndesmosis injuries illustrate how return-to-play thinking differs from traditional care. These injuries require careful evaluation of rotational control and load tolerance before athletes can safely return to sport.
Time alone does not determine readiness. Function determines readiness.
Tools Are Not the System
Students often ask whether I use cupping, scraping, taping, activation work, decompression, or other modalities.
The honest answer is that I use all of them. probably have dozens of variations I use for each tool. My interns and new employees will often tell me, “They like cupping, dry needling, the tools, the vibration.
But the toys are not the system.
Thinking is the system. It’s the art in our professions.

Each tool changes the body in a slightly different way, and each athlete requires a different combination of inputs. The goal is not to use every available modality but to choose the right input at the right time.
OK, now it’s your turn – let’s discuss More cases and Q and A.