A patient walked into the clinic not long ago with a very familiar story:
“I fell on my shoulder wrestling around with some buddies. It’s been a week, and it still hurts to move.”
He had classic symptoms — decreased range of motion, visible hesitation during movement, and a very specific pinpoint area of pain at the top of the shoulder.
And like many patients, he had a clear request:
“Can you do some chiropractic work on it?”
That’s where I had to pause him.
🚧 Not So Fast…
Yes, I’m a chiropractor.
Yes, I work on shoulders all the time.
But doing anything forceful or direct before a real exam would have been irresponsible and potentially harmful.
Why?
Because shoulder pain — especially in active young patients — can come from twenty different sources that all feel the same at first.
Without a proper exam, we’re just guessing. And when it comes to joint integrity, guessing can get people hurt.
✅ Diagnosis: AC Joint Sprain
After a full workup, it was clear this was a low-grade AC joint sprain.
And while he was relieved to hear the words “no surgery” —
he had no clue what the AC joint actually was.
So let’s break it down, SportsDocDC-style:
🦴 What is the AC Joint?
AC stands for acromioclavicular.
It’s the junction where the clavicle (collarbone) meets the acromion, which is the bony hook at the top of your scapula (shoulder blade).
This is the top-front ridge of your shoulder — the spot where pads sit in football or where that bony “bump” appears after trauma.
The AC joint is small — but it’s crucial. It plays a key role in shoulder movement, especially with overhead activity, pressing, pushing, and catching yourself when you fall.
And like all joints held together by ligaments, it can sprain.
🧵 What Is a Sprain, Really?
A sprain is a ligament injury — a structural disruption of the connective tissue that holds two bones together.
Here’s how I explain it in clinic:
Imagine your ligament like an old ACE bandage or a pair of tights.
Over time, with enough force or tension, it can develop a run, like a snag in a sock.
That “run” weakens the fabric — same thing happens with a ligament.
It’s still holding. But now it’s compromised.
📊 Sprains Come in Grades
Sprains aren’t one-size-fits-all. In fact, modern orthopedic classification includes six different types of AC joint separation. But for simplicity — and for the sake of explaining this to athletes and parents — I’m sticking with the classic three-grade system:
Grade 1: Mild Sprain
-
Minor stretch or irritation of the ligament
-
No or only mild visible deformity
-
Localized pain at the tip of the shoulder
-
Still strong and stable
This is what my patient had.
✅ Not surgical. Definitely treatable in clinic.
Painful? Yes.
Limiting? Temporarily.
But with the right treatment plan, it improves quickly and predictably.
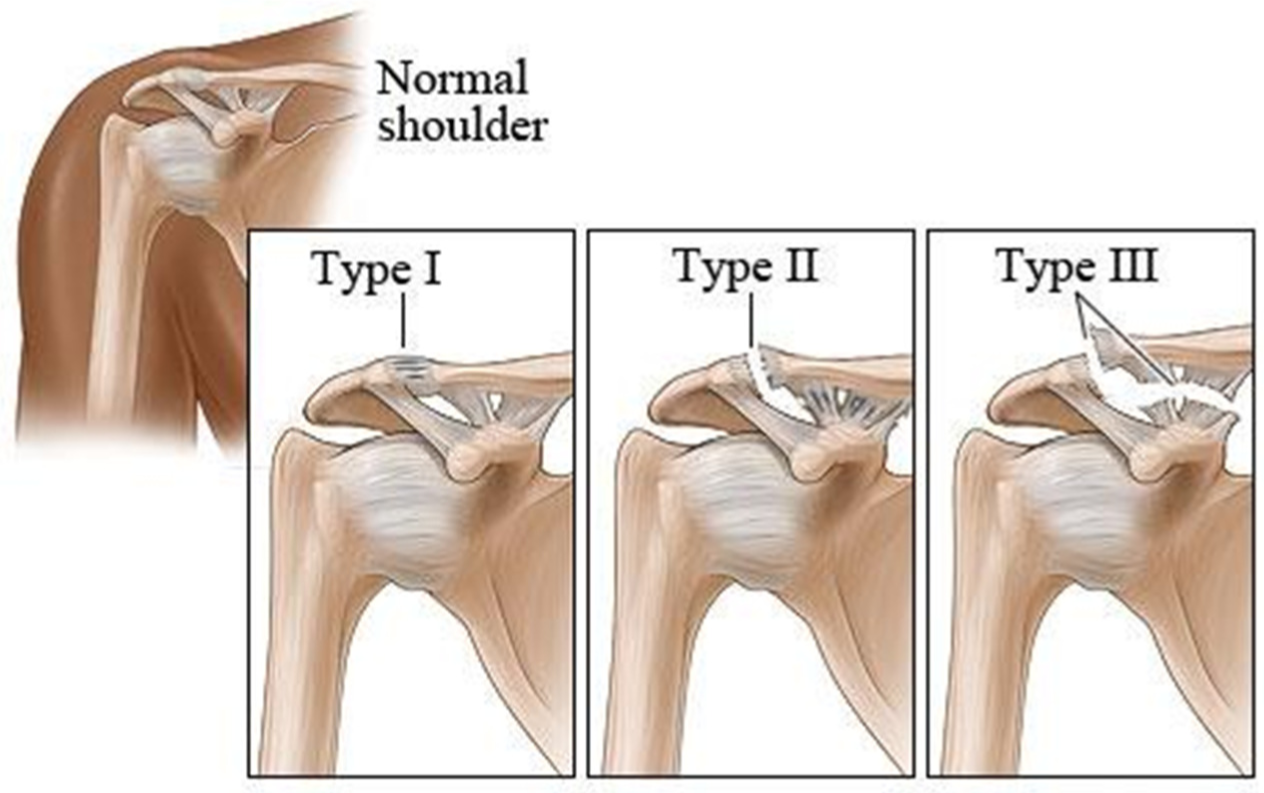
Grade 2: Moderate Sprain
-
Partial tearing of the AC ligaments
-
May see more obvious deformity or a stronger “step sign”
-
Increased weakness or instability during pushing/lifting
-
MRI may be ordered to rule out a complete tear
This is where decision-making starts to vary.
If this were an NFL player in the playoffs?
That’s one pathway.
If it’s a 50-year-old weekend tennis player or coach?
Completely different story.
There’s no single “right answer” here — just smart, personal decision-making based on goals, timing, and risk tolerance.
Grade 3 Severe Sprain (Types IV–VI in modern classification have different bony components as well as the ligament issues):
-
Full tear of the AC and coracoclavicular ligaments
-
Clear “step-off” deformity
-
Significant loss of shoulder function
-
Needs both an MRI and a formal orthopedic evaluation
This is a surgical-grade injury. Period.
This is where you stop guessing and bring in the ortho team.
No more “wait and see.”
No more working around it in the weight room.
This one needs answers, imaging, and a clear plan for recovery — especially if the athlete is planning to return to contact, overhead, or high-demand activity.
🚴 What Makes This Injury Tricky?
The shoulder is an inherently mobile joint — it’s designed to move.
Unlike your hip (a deep ball-and-socket), the shoulder has range over stability.
So when you injure a key stabilizing structure like the AC joint, everyday motions become unpredictable.
You don’t notice it just when lifting weights — you feel it:
-
Buckling when you close the car door
-
Sharp pain pulling a shirt over your head
-
Hesitation during pushups or dumbbell presses
This injury messes with your confidence.
And that’s where good rehab matters.
🧠 How We Treat AC Joint Sprains (Modern Version)
We used to slap on a sling and say “see you in 6 weeks.”
Now, we’re smarter.
Here’s what recovery looks like now:
-
Calm the inflammation.
Early icing, compression, and unloading of the joint. -
Rebuild safe motion.
Scapular mobility work, pain-free pendulums, mid-back movement. -
Control + confidence.
Isometric holds, progressive pushing and overhead transitions. -
Return to load — gradually.
Use a pain scale, not a calendar. The timeline varies. -
Don’t rush overhead work.
Return pressing last, once confidence is back in place.
🧬 Will the Bump Ever Go Away?
Maybe. Maybe not.
A lot of people with moderate AC sprains get a permanent bump at the top of their shoulder.
It’s cosmetic — not a functional limiter.
It’s a battle scar, not a disability.
🔄 Final Word
The AC joint is small — but when injured, it can throw off your whole upper body game.
Recovery isn’t about doing nothing.
It’s about doing the right things, at the right time, in the right sequence.
And it all starts with knowing what you’re dealing with.
It’s the future. Understanding and treatment have changed significantly. This entire website is built to keep you modern.
Don’t let shoulder pain sideline you longer than it should.